
As a nurse, you know how important it is to document patient information accurately and efficiently. That’s where the Nurse Report Sheet comes in handy. This guide will provide you with all the information you need to create an effective Nurse Report Sheet PDF for free.
The first step in creating a Nurse Report Sheet is understanding its important components. From patient demographics to vital signs, each section plays a crucial role in providing a complete picture of the patient’s condition. By familiarizing yourself with these components, you can ensure that your report is comprehensive and informative.
When it comes to writing styles for Nurse Report Sheets, there are several options available. From formal medical language to conversational tone, each style has its own advantages and disadvantages. By choosing the right writing style, you can ensure that your report is clear, concise, and easy to understand.
In addition to understanding the important components of a Nurse Report Sheet and selecting the appropriate writing style, it’s also essential to have access to suitable template examples. DocuKng offers a wide range of templates that can help you create a professional-looking report in no time. By exploring their options, you can find the perfect template for your needs.
Tips on optimizing your Nurse Report Sheet can make all the difference. From using clear and concise language to organizing information effectively, there are several strategies you can use to improve the quality of your report. By following these tips, you can ensure that your report is accurate, complete, and easy to understand.
If you’re looking for a comprehensive guide on creating an effective Nurse Report Sheet PDF for free, look no further than this guide. With information on important components, writing styles, template examples, and optimization tips, you’ll have everything you need to create a professional-looking report that meets your needs.
| Sections | Topics Covered |
|---|---|
| Glossary of Terms | A guide to creating and using nurse report sheets in PDF format. |
| Important Components of a Nurse Report Sheet | The essential elements that should be included in a nurse report sheet. |
| Suitable Writing Styles for Nurse Report Sheets | Different writing styles that are suitable for creating nurse report sheets. |
| DocuKng Template Examples for Nurse Report Sheets | Examples of DocuKng templates that can be used to create nurse report sheets. |
| Tips to Optimize Your Nurse Report Sheet | Advice on how to optimize a nurse report sheet for better organization and efficiency. |
| Common Questions About Nurse Report Sheets | Frequently asked questions about nurse report sheets, including how to fill them out and what information to include. |
Glossary of Terms
Data Normalization: The process of transforming data into a format that can be easily understood and analyzed by machines. In the context of nurse report sheets, this involves organizing patient information in a consistent and structured manner to ensure accuracy and completeness.
Data Encryption: The process of converting plain text into a coded format that is unreadable by unauthorized individuals. In the context of nurse report sheets, this involves ensuring the confidentiality and security of patient information by encrypting sensitive data.
Data Integration: The process of combining data from multiple sources into a single, unified dataset. In the context of nurse report sheets, this involves integrating data from different departments and systems to provide a comprehensive view of patient information.
Data Visualization: The process of creating visual representations of data to facilitate better understanding and decision-making. In the context of nurse report sheets, this involves using charts, graphs, and other visual aids to present complex patient information in an easily digestible format.
Data Mining: The process of analyzing large datasets to identify patterns, trends, and insights. In the context of nurse report sheets, this involves using data mining techniques to extract valuable information from patient records that can inform clinical decision-making.
Important Components of a Nurse Report Sheet
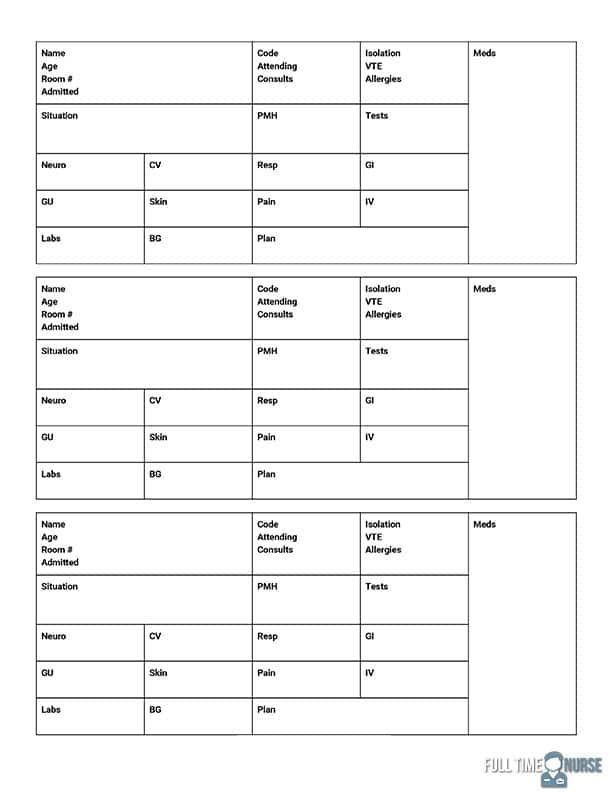
In the fast-paced world of healthcare, nurses play a crucial role in providing quality care to patients. One essential tool that nurses use to document patient information is the nurse report sheet. This document serves as a vital source of information for other healthcare professionals and helps ensure continuity of care. Here, we will discuss the important components of a nurse report sheet.
Patient Information
The first section of the nurse report sheet is typically dedicated to patient information. This includes the patient’s name, date of birth, medical history, and any relevant allergies or sensitivities. It is essential that this information is accurate and up-to-date to ensure that the right care is provided to the patient.
Assessment
The next section of the nurse report sheet is where the nurse documents their assessment of the patient’s condition. This includes observations on the patient’s physical and mental status, as well as any relevant vital signs such as blood pressure, temperature, and pulse rate. The nurse should use clear and concise language to describe the patient’s condition, making it easy for other healthcare professionals to understand.
Plan of Care
The third section of the nurse report sheet is where the nurse outlines the plan of care for the patient. This includes any medications or treatments that the patient is receiving, as well as any goals or objectives for their care. The nurse should clearly document the rationale behind their plan of care and any potential risks or benefits associated with it.
Notes
The final section of the nurse report sheet is where the nurse documents any notes or observations about the patient’s condition. This may include any changes in the patient’s status, any concerns or questions that arise during their care, and any actions taken to address these issues. The nurse should use this section to provide a comprehensive overview of the patient’s care and ensure that all relevant information is documented.
Conclusion
With this, the nurse report sheet is an essential tool for nurses to document patient information and plan of care. The important components of a nurse report sheet include patient information, assessment, plan of care, and notes. By including these elements in their report sheets, nurses can ensure that they provide accurate and comprehensive documentation of the patient’s care.
Suitable Writing Styles for Nurse Report Sheets
In the world of healthcare, nurse report sheets play a crucial role in documenting patient information and medical history. The way these reports are written can have a significant impact on patient care and communication between healthcare professionals. Therefore, it is essential to choose an appropriate writing style for nurse report sheets.
Formal Writing Style
A formal writing style is typically used when reporting critical or sensitive information that requires a high level of accuracy and professionalism. This style is characterized by the use of technical terms, precise language, and a clear and concise structure.
Formal writing style is suitable for nurse report sheets that require detailed medical history, diagnosis, treatment plans, and other critical information. It ensures that the information is presented in a structured manner, making it easy to understand and follow up on patient care.
Informal Writing Style
An informal writing style is more relaxed and conversational, making it suitable for nurse report sheets that require less critical information or when communicating with patients directly. This style is characterized by the use of everyday language, contractions, and a more casual tone.
Informal writing style is ideal for nurse report sheets that focus on patient education, daily care routines, and other non-critical information. It helps to create a personal connection with patients and makes it easier for them to understand the information being presented.
Semantic Writing Style
A semantic writing style is used when reporting information that requires a high level of accuracy but also needs to be easily understood by non-medical professionals. This style is characterized by using simple language, avoiding technical terms, and providing clear explanations for medical jargon.
Semantic writing style is suitable for nurse report sheets that need to be shared with non-medical personnel such as family members or social workers. It ensures that the information is presented in a way that is easy to understand, even for those without a medical background.
Conversational Writing Style
A conversational writing style is characterized by using informal language and a more personal tone. This style is suitable for nurse report sheets that require frequent updates or when communicating with patients in a friendly manner.
Conversational writing style is ideal for nurse report sheets that focus on patient progress, daily activities, and other non-critical information. It helps to create a personal connection with patients and makes it easier for them to understand the information being presented.
DocuKng Template Examples for Nurse Report Sheets
Example 1: Basic Nurse Report Sheet
Patient Name: John Doe
Date of Birth: 01/01/1985
Admission Date: 02/15/2023
Discharge Planned: 02/20/2023
Vital Signs:
* Temperature: 98.6 F (37 C)
* Pulse: 72 bpm
* Respiration Rate: 14 bpm
* Blood Pressure: 125/78 mmHg
* Oxygen Saturation: 95% on room air
Medications:
* Aspirin (81 mg) orally every morning
* Lisinopril (10 mg) orally daily
* Metformin (500 mg) orally twice a day
Allergies: None known
Diagnosis: Hypertension, Type 2 Diabetes Mellitus
Plan:
* Monitor blood pressure and adjust Lisinopril dose as needed
* Encourage regular exercise and healthy diet
* Schedule follow-up appointments with primary care provider and endocrinologist
Example 2: Comprehensive Nurse Report Sheet
Patient Name: Jane Smith
Date of Birth: 07/15/1960
Admission Date: 02/18/2023
Discharge Planned: 02/25/2023
Vital Signs:
* Temperature: 97.8 F (36.6 C)
* Pulse: 64 bpm
* Respiration Rate: 18 bpm
* Blood Pressure: 150/85 mmHg
* Oxygen Saturation: 92% on room air
Medications:
* Lisinopril (10 mg) orally daily
* Metformin (500 mg) orally twice a day
* Atorvastatin (10 mg) orally at bedtime
Allergies: Penicillin, Cephalosporins
Diagnosis: Hypertension, Hyperlipidemia, Type 2 Diabetes Mellitus
Plan:
* Monitor blood pressure and adjust Lisinopril dose as needed
* Encourage regular exercise and healthy diet
* Schedule follow-up appointments with primary care provider and endocrinologist
* Educate patient on proper medication management and adherence
Tips to Optimize Your Nurse Report Sheet
As a nurse, you know how important it is to keep accurate and up-to-date records of your patients’ vital signs, medications, and other health information. One tool that can help you do this is the nurse report sheet.
Choose the Right Format
When it comes to creating a nurse report sheet, there are many different formats to choose from. However, not all formats are created equal. To optimize your nurse report sheet, you should choose a format that is easy to read and understand, as well as one that allows you to input all of the necessary information quickly and accurately.
One popular format for nurse report sheets is the SOAP note format. This stands for Subjective, Objective, Assessment, and Plan. The subjective section includes the patient’s symptoms or complaints, while the objective section includes any relevant observations made by the nurse. The assessment section includes the nurse’s analysis of the patient’s condition, and the plan section includes any recommendations for further treatment or follow-up care.
Keep it Simple
When filling out your nurse report sheet, keep in mind that the goal is to provide a clear and concise summary of the patient’s condition. Avoid using jargon or abbreviations that may be confusing to other healthcare professionals who may read the report.
Use simple language and avoid unnecessary details. Focus on the most important information, such as vital signs, medication schedules, and any changes in the patient’s condition.
Be Consistent
To ensure that your nurse report sheet is accurate and easy to read, it’s important to be consistent in how you fill out the form. Use the same format for each patient, and make sure that all of the necessary information is included on every report.
This will help to reduce errors and ensure that all healthcare professionals have access to the same information about the patient’s condition.
Use Technology
Consider using technology to optimize your nurse report sheet. There are many software programs available that can help you create professional-looking reports quickly and easily. These programs may also include features such as data entry reminders or automatic calculations, which can save you time and reduce errors.
By taking advantage of these tools, you can ensure that your nurse report sheet is accurate, easy to read, and up-to-date with the latest information about your patients’ conditions.
Common Questions About Nurse Report Sheets
How do I make a nurse report sheet?
To create a nurse report sheet, you can use a document template repository like DocuKng or another popular brand that offers customizable templates for employment, business, legal and health-related letters and forms. Simply select the appropriate template, customize it to your needs, and generate the report sheet.
What is nurse brain sheet?
A nurse brain sheet is a document used by nurses to record their observations, assessments, and interventions for patients. It helps them organize their thoughts and ensure they have covered all necessary information.
What is a nursing worksheet?
A nursing worksheet is a tool used by nurses to plan and document patient care. It includes tasks, responsibilities, and goals for each shift.
What should be reported to the nurse?
Any relevant information related to a patient’s health or condition should be reported to the nurse. This includes changes in symptoms, test results, medication side effects, and any other important updates.